
What is Breast Cancer?
Symptoms to look out for
Different types of Breast Cancer
Breast Cancer Diagnosis and Staging
How Breast cancer is treated
Breast cancer is the most common cancer among women.1 About 1.948 million new cases are diagnosed worldwide, and over 513,525 women die of the disease each year.1 This means that one woman is diagnosed with breast cancer somewhere in the world every 20 seconds and more than three women die of breast cancer every five minutes worldwide.1
Since 2008 there has been a 22 percent increase in the number of people developing breast cancer worldwide. The good news is that despite this increase, there has been a significant drop in the number of deaths from the disease. This decrease can be attributed to a combination of factors such as better understanding of the disease, earlier diagnosis, improved testing and effective treatments.
Despite the significant progress made over the last few decades in patient outcomes, breast cancer is still the most common cancer affecting women. Every 20 seconds a person is diagnosed with breast cancer and every minute someone dies of this disease.
These sobering facts underscore the importance of continuous investment in this field. Whilst investment in research and the development of new treatments play a critical role in improving patient outcomes, one should not undermine the importance of education and general awareness about the disease. When it comes to breast cancer, knowledge is not only power, but it may also be a life saver.
October is Breast Cancer Awareness Month (BCAM) which provides an excellent opportunity to remind ourselves just how important awareness is in our common battle against the disease. Awareness built on a simple but proven premise that can change lives: greater knowledge and awareness = earlier detection = increased survival rates.
Greater knowledge of the risk factors for breast cancer, the symptoms to look out for and seeking advice as early as possible make the detection and treatment of the disease at the early stages possible. If the cancer is found before it has spread, 98 percent of people live for at least five years, compared to just 24 percent when the cancer is diagnosed at a later stage




- Symptoms to look out for
- Types of breast Cancer
- What is breast cancer staging?
- How breast cancer is treated
A hard lump developing in the breast or armpit – typically painless and occurring on one side only.
- A change in the size or shape of the breast, including indentation, ‘growing’ (particularly prominent) veins or skin loss.
- Changes in the skin such as hardening, dimpling, bumps, redness/heat or an orange peel like appearance.
- Changes in the nipple such as retraction, the secretion of unusual discharge or a rash around the nipple area.

Contrary to common belief, breast cancer is not just one disease
There are several types of breast cancer, which can be classified based on the proteins (known as receptors) that coat the surface of the cancer cells. These proteins play an important role in tumour development, by signalling cells to grow and divide.
Knowing the type of breast cancer, a patient has helps determine the most effective treatment approach and the likely course of the illness
Each type of breast cancer is identified by the presence or absence of three receptors found on the surface of cells: the oestrogen receptor (ER), the progesterone receptor (PR) and the Human Epidermal Growth Factor Receptor 2 (HER2).2 When diagnosed, people can be confirmed as being positive or negative for more than one of these receptors.
Hormone Receptor (HR)-positive breast cancer
HR-positive breast cancer is the most common type of breast cancer, accounting for approximately 80% of cases.2 Breast cancers are considered HR-positive when tumour cells produce abnormal amounts of receptors for the hormones, oestrogen and/or progesterone. As these hormones signal cells to grow and divide, having too many receptors on the surface of a cell can cause uncontrolled growth and the formation of a tumour. HR-positive breast cancers are commonly treated with medicines, known as hormone therapies, that block the activity of ER and/or PR, or that reduce hormone levels. within the HR+ population there are tumors that have low levels of HER2 expression called HER2Low for which this HER2 receptor may still be targetable HER2-low category includes those who have IHC scores of 1+ and 2+ without amplification (as measured by that FISH test).
HER2-positive breast cancer
HER2-positive breast cancer – characterised by cells that over-produce the HER2 protein – represents approximately 20% of all breast cancers. This type of breast cancer can be particularly aggressive. If left untreated, it is associated with faster disease progression and poorer chances of survival compared to HER2-negative disease (i.e. breast cancer cells that are coated with normal amounts of the HER2 protein). Today, treatments are available that specifically target HER2, blocking the signals that cause cancer cells to grow and multiply.
Triple-negative breast cancer
Triple-negative breast cancer (TNBC) is a rare form of breast cancer, accounting for around 10-20% of all breast cancers. It is a type of breast cancer that lacks oestrogen and progesterone receptors and does not over-produce the HER2 protein. The mechanisms that drive this type of cancer are therefore largely unknown, which makes it a particularly difficult type of breast cancer to treat. Although patients may respond to chemotherapy, overall, treatment options are limited, and the prognosis is often poor.5 there are TNBC tumours that have low levels of HER2 expression called HER2Low for which this HER2 receptor may still be targetable, HER2-low category includes those who have IHC scores of 1+ and 2+ without amplification (as measured by that ISH test).
Knowing the type of breast cancer, a patient has is important, because whilst some treatments such as surgery and radiotherapy may be similar across different types of breast cancer, drug treatments such as chemotherapy, hormonal therapy and targeted therapies will differ between cancer types.
Breast cancer is also diagnosed and treated according to its ‘stage’
When diagnosed, patients will be told the ‘stage’ of their breast cancer. This indicates how big it is and how far it has spread (if at all). The stage is important because it helps cancer specialists to decide on the best course of treatment for a patient. Generally, the more advanced the cancer is, the harder it is to treat and the worse the prognosis is likely to be.

Staging is a way of describing how extensive the breast cancer is, including the size of the tumor, whether it has spread to lymph nodes, whether it has spread to distant parts of the body, and what its biomarkers are.
Staging can be done either before or after a patient undergoes surgery. Staging done before surgery is called the clinical stage, and staging done after surgery is called the pathologic stage. Doctors use diagnostic tests to find out cancer’s stage, so staging may not be complete until all of the tests are finished. Knowing the stage helps the doctor recommend the best kind of treatment and can help predict a patient’s prognosis, which is the chance of recovery. There are different stage descriptions for different types of cancer.
TNM staging system
The most common tool that doctors use to describe the stage is the TNM system. Doctors use the results from diagnostic tests and scans to answer these questions:
- Tumor (T): How large is the primary tumor in the breast? What are its biomarkers?
- Node (N): Has the tumor spread to the lymph nodes? If so, where, what size, and how many?
- Metastasis (M): Has the cancer spread to other parts of the body?
The results are combined to determine the stage of cancer for each person.
There are 5 major stages of breast cancer: stage 0 (zero), which is non-invasive ductal carcinoma in situ (DCIS), and stages I through IV (1 through 4), which are used for invasive breast cancer. The stage provides a common way of describing the cancer, so doctors can work together to plan the best treatments. (JCC Cancer Staging Manual, Eighth Edition – 2017)
DCIS is a non-invasive cancer, but if not removed, it may develop into an invasive breast cancer later. DCIS means that cancer cells have been found in breast ducts and have not spread past the layer of tissue where they began
Staging can be clinical or pathological. Clinical staging is based on the results of tests done before surgery, which may include physical examinations, mammogram, ultrasound, and MRI scans. Pathological staging is based on what is found during surgery to remove breast tissue and lymph nodes. The results are usually available several days after surgery. In general, pathological staging provides the most information to determine a patient’s prognosis.
Early breast cancer (eBC) and advanced breast cancer (aBC)
The majority of breast cancer cases are diagnosed at an early stage, before the cancer has spread beyond the breast. When treated at this early stage, breast cancer may be potentially curable. The eBC treatment approach is comprehensive and may involve treatment before and after surgery to remove the cancerous cells and prevent them from returning.
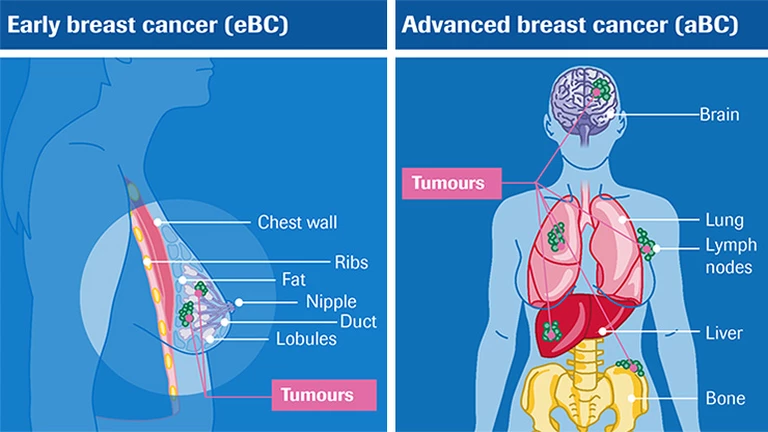
Unfortunately, some patients are initially diagnosed with an advanced stage of disease, or they see their cancer return and worsen after initial treatment for eBC. For patients whose cancer has spread to other parts of the body, such as the brain or liver. The goal of treatment for patients with aBC is to prolong life as much as possible, while also trying to keep patients feeling as well as possible by managing symptoms and treatment side effects.
Diagnosing and treating breast cancer early, before it has spread may provide the best chance of cure.
In cancer care, doctors specializing in different areas of cancer treatment—such as surgery, radiation oncology, and medical oncology—work together with radiologists and pathologists to create a patient’s overall treatment plan that combines different types of treatments. This is called a multidisciplinary team. Cancer care teams include a variety of other health care professionals, such as physician assistants, nurse practitioners, oncology nurses,.
The biology and behavior of breast cancer affects the treatment plan. Some tumors are smaller but grow quickly, while others are larger and grow slowly. Treatment options and recommendations are very personalized and depend on several factors, including:
- The tumor’s subtype, including hormone receptor status (ER, PR), HER2 status, and nodal status
- The stage of the tumor
- Genomic tests,
- The patient’s age, general health, menopausal status, and preferences
- The presence of known mutations in inherited breast cancer genes, such as BRCA1or BRCA2, based on results of genetic tests
For both ductal carcinoma in situ (DCIS) and early-stage invasive breast cancer, doctors generally recommend surgery to remove the tumor. To make sure that the entire tumor is removed, the surgeon will also remove a small area of healthy tissue around the tumor, called a margin.
Although the goal of surgery is to remove all of the visible cancer in the breast, microscopic cells can be left behind. In some situations, this means that another surgery could be needed to remove remaining cancer cells.
There are different ways to check for microscopic cells that will ensure a clean margin. It is also possible for microscopic cells to be present outside of the breast, which is why systemic treatment with medication is often recommended after surgery, as described below.
For larger cancers, or those that are growing more quickly, doctors may recommend systemic treatment with chemotherapy, immunotherapy, and/or hormonal therapy before surgery, called neoadjuvant therapy. There may be several benefits to having drug treatments before surgery:
- Surgery may be easier to perform because the tumor is smaller.
- Your doctor may find out if certain treatments work well for the cancer.
- You may be able to try a new treatment through a clinical trial.
- If you have any microscopic distant disease, it will be treated earlier by the drug therapy that circulates through the body.
- People who may have needed a mastectomy could have breast-conserving surgery (lumpectomy) if the tumor shrinks enough before surgery.
After surgery, the next step in managing early-stage breast cancer is to lower the risk of recurrence and to try to get rid of any remaining cancer cells in the body. These cancer cells are undetectable with current tests but are believed to be responsible for a cancer recurrence, as they can grow over time. Treatment given after surgery is called “adjuvant therapy.” Adjuvant therapies may include radiation therapy, chemotherapy, targeted therapy, immunotherapy, and/or hormonal therapy (see below for more information on each of these treatments).
Whether adjuvant therapy is needed depends on the chance that any cancer cells remain in the breast or the body and the chance that a specific treatment will work to treat the cancer. Although adjuvant therapy lowers the risk of recurrence, it does not completely get rid of the risk.
Along with staging, other tools can help estimate prognosis and help you and your doctor make decisions about adjuvant therapy. Depending on the subtype of breast cancer, this includes tests that can predict the risk of recurrence by testing your tumor tissue (such as Oncotype Dx™ or MammaPrint™; see Diagnosis). Such tests may also help your doctor better understand whether chemotherapy will help reduce the risk of recurrence.
If surgery to remove the cancer is not possible, it is called inoperable. The doctor will then recommend treating the cancer in other ways. Chemotherapy, immunotherapy, targeted therapy, radiation therapy, and/or hormonal therapy may be given to shrink the cancer.
For recurrent cancer, treatment options depend on how the cancer was first treated and the characteristics of cancer mentioned above, such as ER, PR, and HER2.

References
- Globocan 2022 [Online]. Available from: http://globocan.iarc.fr [Accessed Sep 2022].
- WebMD, Types of Breast Cancer: ER Positive, HER2 Positive, and Triple Negative. [Online]. Available from: http://www.webmd.com/breast-cancer/breast-cancer-types-er-positive-her2-positive [Accessed 6 September 2016].
- Wolff AC, et al. Journal of Clinical Oncology 2013;31(31):3997-4013.
- National Breast Cancer Foundation, Triple Negative Breast Cancer [Online]. Available from: http://www.nationalbreastcancer.org/triple-negative-breast-cancer [Accessed 12 September 2016]
- Cancerhelp.org. Triple Negative Breast Cancer. [Online]. Available from: http://www.cancerhelp.org.uk/about-cancer/cancer-questions/triple-negative-breast-cancer [Accessed 2 September 2016].
- Hammond E. Journal of Clinical Oncology 2011;29,15:e458.
- Cancer Research UK [Online]. Survival statistics for breast cancer. Available from: http://www.cancerresearchuk.org/about-cancer/type/breast-cancer/treatment/statistics-and-outlook-for-breast-cancer [Accessed 12 September 2016].
- Howlader N, et al. [online]. SEER Cancer Statistics Review (CSR). Available from: http://seer.cancer.gov/csr/1975_2011/ [Accessed 30 March 2015].
- Cardoso F, et al. Annals of Oncology 2012; 23(suppl 7):vii11-9.
- Cancer Research UK [Online]. Why is early diagnosis important? Available from: http://www.cancerresearchuk.org/about-cancer/cancer-symptoms/why-is-early-diagnosis-important [Accessed 12 September 2016].
- Cardoso F, et al. Annals of Oncology 2014;25:1871–1888.